
01 · Daily · low impact
Walk, Swim, or Cycle
Daily low-impact movement is the foundation. Aim for 20–40 minutes most days. Swimming is ideal during flares because the water unloads the joint.
20–40 min, 5×/week
The menopause-aware playbook for hip pain — a self-check quiz, daily strengthening routine, supplements, sleep fixes, and the medical interventions worth exploring. Built by Dr. Tammy for the women whose joint pain medicine keeps calling just aging.
Instant PDF · No spam · Unsubscribe anytime

"Your hips know the hormone story. Medicine just hasn't caught up."
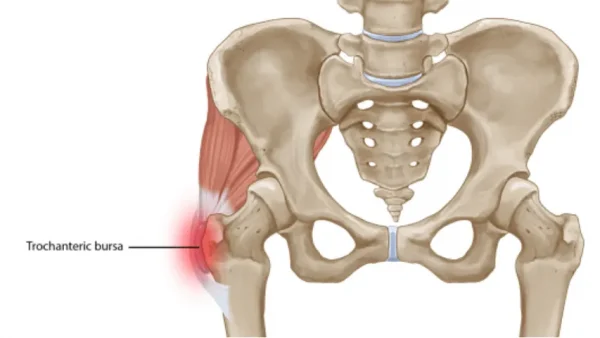
Estrogen protects bone density, regulates collagen in tendons and cartilage, lubricates the joint, and damps inflammation. When it drops in perimenopause and menopause, the hip — your biggest weight-bearing joint — takes the hit. Gluteal tendons get irritable, the bursa flares, cartilage wears faster, and bone density falls (by up to 20% in the years around the final period).
Collagen — the protein in every tendon, ligament, and cartilage surface — depends on estrogen for synthesis and repair. The gluteal tendons attach to the outer hip and are especially estrogen-sensitive, which is why postmenopausal women have disproportionately more gluteal tendinopathy, trochanteric bursitis, and outer-hip pain than men of the same age.
The first two are red-flag questions — hip pain can also mean a fracture or infection. Answer honestly. Not a diagnosis.
Start with low-impact aerobic movement to warm the joint. Strengthen the glutes before you stretch. Stop short of sharp pain — especially with bursitis. If a movement flares the outer hip for more than 24 hours, regress the load.
Daily low-impact movement is the foundation. Aim for 20–40 minutes most days. Swimming is ideal during flares because the water unloads the joint.

Side-lying with knees bent and a light loop band above the knees. Open the top knee like a clam without rolling your pelvis backward. Targets the gluteal tendons that estrogen loss weakens first.

On your back, knees bent, feet flat. Squeeze your glutes and lift your hips into a straight line. Pause at the top. Builds posterior chain without loading the joint.

Hold a chair for balance. Keep your toes pointing forward and lift the leg straight out to the side without leaning. Lower with control.

Hold a chair. Keep the leg straight and slowly press it back behind you, squeezing the glute. Don't arch your low back. Counters seated-day glute amnesia.

Sitting or lying down, cross one ankle over the opposite knee and gently lean forward (or pull the bottom thigh toward you). Opens the deep hip rotators that compress the sciatic nerve.
None of these regrow cartilage. They reinforce the connective tissue and bone that estrogen used to look after. Run any new supplement past your doctor — especially with blood thinners, diabetes meds, or thyroid medication.
Professional-quality brands at member pricing through our Fullscript portal.
Open supplement portalFoundational for bone density. Test 25-OH-D before megadosing.
Prefer dietary sources. Supplement only the gap.
Supports tendon and cartilage repair. Pair with vitamin C.
Reduces joint inflammation and protects cartilage.
Muscle relaxation, sleep, bone matrix.
Comparable to NSAIDs in some osteoarthritis trials.
Modest but real effect on osteoarthritis symptoms.
Supports estrogen metabolism and bone mineralization.
Small pillow under the knees keeps the pelvis neutral and offloads the gluteal tendons.
Hug a body pillow between your knees and ankles so the top leg stays stacked — no internal rotation pulling on the outer hip.
Direct pressure compresses the bursa and tendons. The #1 reason outer-hip pain wakes you up.
Letting the top knee fall to the mattress yanks the gluteal tendons all night. Use a pillow between the knees.
Ordered roughly by evidence and where most people start. Don't skip ahead to hip arthroscopy before you've tried 12 weeks of glute-focused PT and load management.
A PT trained in pelvic/hip biomechanics. 6–12 weeks of glute-medius and posterior-chain work before judging results.
Best evidence when started under 60 and within 10 years of menopause. May ease joint pain and protect bone — discuss as a joint conversation, not just hot flashes.
Stop sleeping on the painful side, swap deep squats and lunges for hip-hinges, and avoid crossing your legs while sitting. The single biggest lever for bursitis and tendinopathy.
Short courses for flares. NSAIDs reduce bursitis pain and swelling. Use the lowest dose for the shortest time, with food.
Useful for bursitis flares when PT alone isn't moving things. Limit to a small number per joint per year.
Baseline bone-density scan around menopause. Catches osteoporosis before a fracture happens — not after.
X-ray rules in/out hip osteoarthritis. MRI is the gold standard for gluteal tendinopathy and labral pathology.
Good evidence for gluteal tendinopathy and greater trochanteric pain syndrome. Multiple sessions, non-invasive.
Growing evidence for chronic gluteal tendinopathy. Better long-term outcomes than cortisone in some trials.
For labral tears or impingement. Specialist territory — get a hip-preservation surgeon, not a general orthopedist.
Decent evidence for chronic hip pain and piriformis syndrome, especially paired with PT.
Eases compensatory tightness in the IT band, TFL, and lumbar paraspinals that pile on once the hip starts hurting.
If you'd like support with hormone therapy and menopause or perimenopause hormone restoration, book a free call with our team.
Instant PDF · No spam · Unsubscribe anytime